



Carilion Clinic is a not-for-profit health care organization based in Roanoke, VA. In line with their mission to improve the health of the communities they serve, and with the intent of becoming a teaching facility, Carilion Clinic set upon upgrading their operating rooms and related existing HVAC systems at the Carilion New River Valley Medical Center in Christiansburg, VA.
Designed in the mid-1990s, the existing HVAC systems were not suited to meet the increasing demands and expectations from the surgical staff. The engineering team from SmithGroupJJR was tasked with designing new HVAC systems for the operating rooms that meet the current and future needs of the surgical staff. Carilion Clinic was looking to improve the efficiency and flexibility of the operating rooms. The requests from the surgical staff were unique from a mechanical viewpoint and led to many challenges in the design process. For example, the staff wanted to book their procedures on a completely flexible schedule, meaning the same room could see a pediatric surgery immediately followed by an orthopedic surgery.
Design for the major renovation began with the endusers in mind. It was important that the new operating room HVAC system work seamlessly with the staff during their complex surgical procedures. In order to create this seamless system, the Carilion surgical staff was interviewed to learn all about their working routines before, during, and after surgery. These conversations provided tremendous insight into how the HVAC system could make their working routines easier, more efficient, and more comfortable. Their requests and insights eventually drove the mechanical system design as described throughout the rest of this article.
Managing Time And Space
Each doctor had different temperature and humidity preferences for their varying procedure types. And for good reason, too — they were very well researched in the effects of operating room temperature and humidity on the human body during open surgery. Some procedures, such as pediatric and vascular, are better performed in a warm and humid environment. Out of these climate conditions, the extreme we received was 80ºF/50% rh.
On the other hand, some procedures, such as orthopedics surgery, called for colder environments because the doctors wear heavy and thick gear throughout the entire procedure. The extreme climate condition desired on this end of the spectrum was 64ºF/30% rh.
Figure 1 charts the entire range of desired climate conditions we discovered from polling the surgical staff. Compared to the range of conditions suggested by ASHRAE Standard 170, the doctors actually requested a larger spread. ASHRAE Standard 170-2013, as part of the 2014 FGI Guidelines, lists 68º to75ºF, 20% to 60% rh for Class B and Class C operating rooms. The lesson here is that ASHRAE Standard 170 provides a great starting point for temperature and humidity design conditions, but it is important to also consider the endusers. If the new mechanical system had been sized to achieve the range of set points listed in ASHRAE Standard 170, some of the doctors would not have received their desired conditions.
Air at the low-climate condition (64ºF/30% rh) has a 32ºF dew point temperature. It is not possible to cool to that level with a standard chilled water system, nor is it feasible with a glycol solution. We had to look to other cooling and dehumidification methods to achieve supply air conditions that can maintain the low-climate condition. Desiccant dehumidification was selected because it could reach the desired supply dew points while minimizing the project impact on the existing hospital facility.
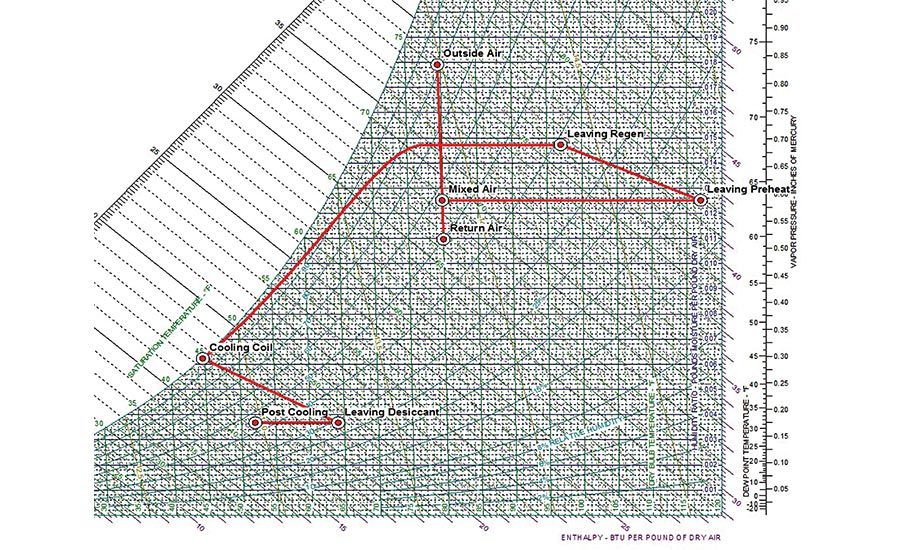
The final system was able to achieve all desired supply air conditions with the existing utilities already available throughout the hospital. The facility staff appreciated the efforts to minimize the project impact on the rest of the hospital systems. Heating, desiccant preheat, and reheat are all done with hot water from the hospital campus main boiler plant. Campus chilled water serves the cooling coils and post-cooling coils. Finally, humidification steam is provided by the campus steam boiler plant. Plant temperatures and set points did not need to change at all due to our new design. Figure 2 shows the peak sizing psychrometrics of the designed system, while Table 1 lists out the properties of each point on the graph.
From first glance, it appears that this system is slightly oversized since there is a difference between the supply air and return air conditions. However, this difference was intentional in the peak sizing exercises. In between surgeries, sterilization and prep occurs to changeover the room for the next procedure. The Carilion staff reported that their sterilization process is like a well-oiled machine. Total changeover time could take as little as 10 minutes. The operating rooms are flexibly scheduled, with procedures based on room and doctor availability. Each operating room is not dedicated to a specific procedure type.
This places an interesting challenge on the HVAC design. Consider the scenario where a procedure operates at the high-climate condition (80ºF/50% rh) and then is immediately followed by a procedure at the low-climate condition (64ºF/30% rh) just 10 minutes later. The system has to be sized at peak to handle this rapid and drastic changeover. Our goal was to provide the surgical staff their desired climate conditions throughout the entire surgery, including the start of the procedure.
In most HVAC applications, the cooling coil is sized to bring a mixture of return air and outdoor air down to a state that can maintain equilibrium in the current room conditions. Not so in this case. The cooling coil in the new Carilion systems had to be sized in order to quickly satisfy any changes in the desired set points such that dehumidification is achieved to meet the lowest operating room relative humidity setpoint. Thus, the large difference in return air and supply air conditions in our peak system sizing shown in Figure 2 and Table 1. Even though one air handling unit served multiple operating rooms, the zone humidifiers and related hot water reheat coils located at the terminal unit level allowed each operating room to have its own climate conditions.
Added Controls Help
The vision we shared with Carilion is that the temperature and humidity set points would be changed during the sterilization and prep process, and the mechanical system would achieve equilibrium at the new set points by the start of the next procedure. In order to make this process as seamless as possible, the control panel interface was made to be a touchpad at the door of each operating room. The interface can host preset climate conditions per doctor or per procedure type. These preset climate condition set points can be switched over to the next desired conditions with only one touch at the control pad. Time saved from messing with the temperature and humidity controls can be refocused on the sterilization process.
The control touchpad system also constantly monitors the room pressurization. Operating room pressurization at the Carilion medical center is directly monitored with DP sensors, and controls actively adjust the relative pressure in the room with supply and return air valves. Figure 3 shows the controls diagram at the operating room level.
Room pressurization controls for operating rooms should be able to monitor and actively adjust the room pressurization. There are legal and financial consequences if the pressurization system fails to maintain differential pressure. In the Carilion controls system, we installed a check in the controls sequence to report the differential airflow through the supply and return air valves. It is easy to verify that the DP sensors are working correctly if a positive airflow differential is reported along with a positive differential pressure.
The Carilion surgical staff also told us about their processes for recording climate conditions during each procedure. We saw an opportunity to save effort on their behalf by automating that recording process. A separate trendlog file is recorded by the controls system for each procedure with relative pressure, temperature, and humidity data. That file is automatically saved into a database, eliminating the manual recording process.
Finally, there are some other design details not listed above that are worth mentioning. The existing HEPA filters were installed locally at the supply inlet of each operating room, but were relocated to be installed in the new air handling units at the overall system level. The maintenance staff reported that it was difficult to change the HEPA filters above the ceiling of a working surgical suite corridor. The three new AHUs were headed together with bypass isolation dampers to give the hospital some flexibility in taking down units for maintenance. It does not create a true N+1 arrangement, but the arrangement allows the hospital to continue using the operating rooms connected to a downed AHU in emergency situations. Figure 4 shows the duct heading with isolation dampers.
Conclusion
As designers, it is not enough to just have good technical skills to make a project successful. We need to hear, listen, and understand a client’s demands and expectations. The intent of the article is not to brag about the system, but to celebrate the success of a project that could not have been done without approaching issues from an overall system level and by listening to the endusers.
User experience input was invaluable throughout this process. Had Carilion Clinic decided to simply fix the known issues, the result would have been a system at just an acceptable level. Instead, they received a mechanical and controls system that works seamlessly and meets the demands and expectations of the surgical staff. Together, we were able to create a new mechanical system that increases their overall operating efficiency, provides all climate conditions desired by the doctors, and serves the facility without straining their existing systems. Carilion New River Valley Medical Center fulfilled their vision of having an operating room of the future. ES








